The thalassaemias
The thalassaemias are a heterogeneus group of inherited disorders of haemoglobin synthesis. They are characterised by a reduction in the rate of synthesis of either alpha or beta chains and are classified accordingly. Unbalanced synthesis of alpha and beta-globin chains can damage red cells.
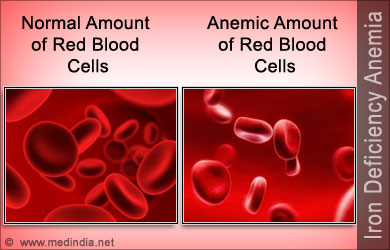
The basic haematological abnormality is a hypochromic microcytic anaemia of variable severity. The clinical severity of any thalassaemia is proportionate to the degree of imbalance of alpha and beta-globin chain synthesis.

α-Thalassaemias:
-Hb-Barts hydrops syndrome: there is a complete absence of α-chain synthesis which is needed for fetal and adult haemoglobin, the disorder is incompatible with life and death occurs in utero.
-HbH disease: there is a moderate chronic haemolytic anaemia with splenomegaly and sometimes hepatomegaly. Severe bone changes and growth retardation are unusual.
-α-Thalassaemia traits (carrier state).
β-Thalassaemias:
-β-Thalassaemia major: the characteristic severe anaemia is caused by α-chain excess leading to ineffective erythropoiesis and haemolysis. Anaemia first becomes apparent at 3-6 months, child fails to thrive and develops hepatosplenomegaly. Compensatory expansion of the marrow spaces causes atypical facies with skull bossing and maxillary enlargement. If left untreated further complications can include repeated infections, bone fractures and leg ulcers.
Blood transfusion remains the mainstay of management, splenectomy can reduce its frequency. With such regular transfusion iron chelation is necessary to minimise iron overload (accumulation of iron damages the liver, endocrine organs and heart with death), the common regimen is subcutaneous desferrioxamine given for 5-7 days per week. Compliance may be problematic but where good there is a considerably improved life expectancy.

-Thalassaemia intermedia: the clinical features are less severe than in β-Thalassaemia major. Patients usually present later (often at 2-5 years), have relatively high haemoglobin levels, moderate bone changes and normal growth. Regular transfusion is not required.
-β-Thalassaemia trait (minor): is a symptomless clinical disorder which should not be confused with iron deficiency. Genetic counselling is required in selected patients.
Sickle cell syndromes
The sickle cell syndromes are a group of haemoglobinopathies which primarily affect the Afro-Caribbean population. The common feature of these diseases is inheritance of an abnormal haemoglobin beta-chain gene, inheritance of two of these abnormal genes leads to a serious disorder termed sickle cell anaemia.

Sickle cell anaemia (HbSS): the classic form of sickle cell syndrome is enormously variable in severity.
-Haemolytic anaemia: the haemoglobin is usually in the range 60-100g/L, the symptoms of anemia are often surprisingly mild. Intercurrent infection with parvovirus or folate deficiency can cause a sudden fall in haemoglobin ("aplastic crisis").
-Vascular-occlusive crises: acute, episodic, painful crisis are a potentially disabling feature of sickle cell anemia. They may be triggered by infection or cold. Patients complain of musculoskeletal pain, hips, shoulders and vertebrae are most affected. Attacks are generally self-limiting but infarction of bone can occur. Other organs are vulnerable to infarction; most serious neurological damage which may manifest as seizures, transient ischaemic attacks and strokes. Vaso-occlusion in infancy is responsible for the "hand-foot syndrome", a type of dactylitis damaging the small bones of hand and feet.

First line treatment is rest, increased fluids and adequate oral analgesia. Constitutional upset or pain not relieved by oral analgesia requires hospital admission with continued rest, warmth, intravenous fluids and opiate analgesia.
-Sequestration crises: these arise from sickling and infarction within particular organs. Specific syndromes include "acute chest syndrome" with occlusion of the pulmonary vasculature, "girdle sequestration" caused by occlusion of the mesenteric blood supply, and hepatic and splenic sequestration.
-other complications: papillary necrosis with haematuria, loss of ability to concentrate urine, nephrotic syndrome, priapism, lower limb ulceration, proliferative retinopathy, glaucoma, liver damage and pigment gallstones.
Management:
Prophylaxis is important, patients should avoid factors known to precipitate crisis, take folate supplements and be prescribed penicillin and pneumococcal vaccine. Infections require prompt treatment.
Treatment options are blood transfusions, hydroxycarbamide and stem cell transplantation when indicated.
Prognosis:
The risk of early death is inversely related to fetal haemoglobin levels. The most common causes of death are infection in infancy, cerebro-vascular accidents in adolescence and respiratory complications in adult life.
Sickle cell trait (HbAS): normally causes no clinical problems. However, haematuria occasionally occurs as a result of renal papillary necrosis and additional care is required during pregnancy and anaesthesia.
Sources:
-http://www.slideshare.net/giridharkv/thalassemia-drkvgiridhar
-https://www.pinterest.com/kedillard/thalassemia-awareness/
-Haematology, 3rd Edition, Martin R. Howard, Churchill Livingstone, Elsevier, 2008.
-https://www.linkedin.com/pulse/sickle-cell-disease-scd-metrohealth-hmo
-http://www.slideshare.net/sandipgupta77770194/sickle-cell-disease-sandip







.jpg)








.jpg)